Robotic D2 Total Gastrectomy with Station 10 Lymph Node Dissection
Introduction
Robotic-assisted gastrectomy (RAG) is slowly gaining acceptance in the treatment for gastric cancer. Due to its recent adoption for gastrectomy in Singapore, robotic experience is still lacking. The indications for RAG are similar to those of conventional laparoscopic surgery. Locally advanced tumours are usually excluded from minimally invasive surgery1.
Compared with conventional laparoscopic surgery, RAG offers more precise lymphadenectomy by providing several technical advantages, such as motion scaling, tremor filtering, articulated endoscopic wrist with improved dexterity and three-dimensional imaging2.
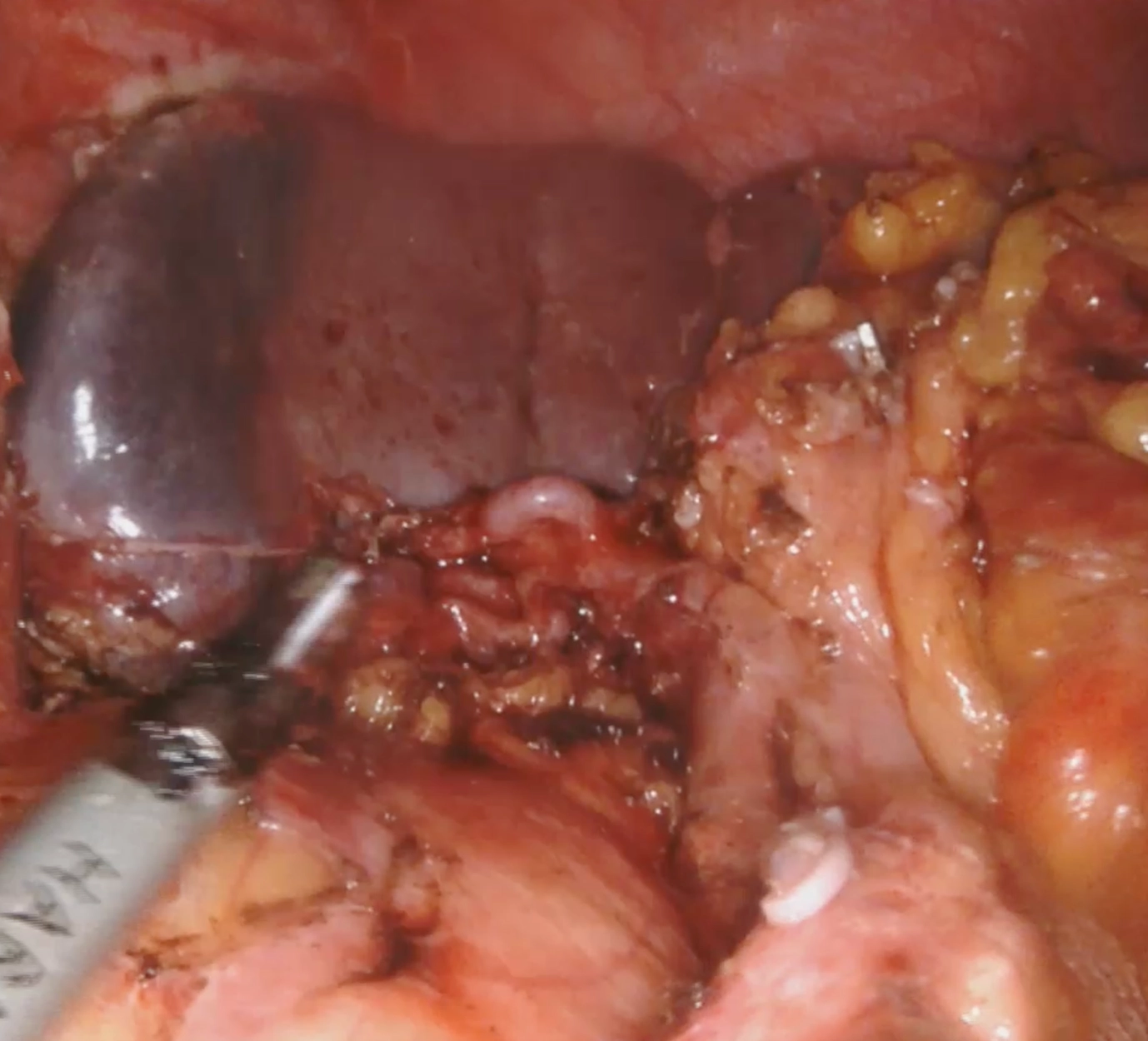
We present a case of robotic D2 total gastrectomy for a locally advanced gastric fundal tumor with enlarged lymph nodes along the splenic artery. Mdm U is a 53year old female who underwent gastroscopy for anemia, and a tumor was noted at the fundus. Histology was adenocarcinoma. Computed tomographic scan of the thorax/abdomen/pelvis showed a lesion involving the gastric fundus and enlarged lymph nodes adjacent to the upper stomach, celiac axis and along the splenic artery.
Methods
The patient is positioned in supine with both arms out. Ports are placed in a V-shaped fashion, with 8mm ports for the robotic instruments and a 12mm port in the left mid-clavicular line for the assistant. We utilize the Maryland bipolar in the 1st arm, Harmonic ultrasonic shears in the 2nd arm, and Cadiere forceps in the 3rd arm. The oesophagojejunostomy and jejuno-jejunostomy anastomosis were created with Signia(Medtronic) staplers.
Results
Surgery time was 480minutes and blood loss was 50mls. Intra-op findings was a 7x6cm tumour at the fundus, with enlarged lymph nodes along station 8, 11p and 11d. Final histology was Stage IIA, T3 tubular adenocarcinoma, N0 (0/54 lymph nodes), margins clear. Patient tolerated soft diet by post-operative day (POD) 5 and was discharged home on POD 7.
Conclusion
RAG is a safe and feasible procedure that allows adequate lymph node harvest and R0 resection with low post-operative morbidity. For surgeons with sufficient experience in laparoscopic surgery, the learning curve of RAG is shorter3. With the advancement of robotic technology and surgeons’ experience, the indications of RAG can be extended to include advanced gastric cancer.
Reference
- Japanese Gastric Cancer A. Japanese Gastric Cancer Treatment Guidelines 2021 (6th edition). Gastric Cancer 2023; 26(1): 1-25.
- Song J, Oh SJ, Kang WH, Hyung WJ, Choi SH, Noh SH. Robot-assisted gastrectomy with lymph node dissection for gastric cancer: lessons learned from an initial 100 consecutive procedures. Ann Surg 2009; 249(6): 927-32.
- Alhossaini RM, Altamran AA, Seo WJ, Hyung WJ. Robotic gastrectomy for gastric cancer: Current evidence. Ann Gastroenterol Surg 2017; 1(2): 82-9.