A Multi-Nozzle Nebulizer Does Not Improve Tissue Drug Delivery During PIPAC
Authors
Iaroslav Sautkin, Juergen Weinreich, Marc A. Reymond
Affiliations
National Center for Pleura and Peritoneum, University Hospital Tübingen, Germany
Introduction
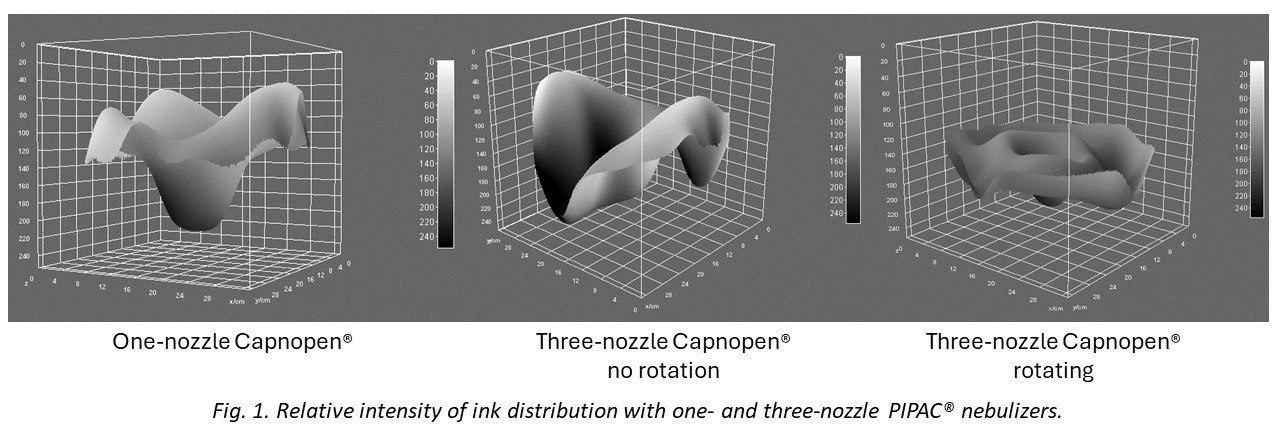
After PIPAC with the Capnopen® (Capnopharm, Tübingen, Germany), heterogeneous drug distribution was reported. To improve drug distribution, we developed a three-nozzle nebuliser (“Triplepen”) and compared the performance of both devices ex-vivo.
Methods
In physical experiments, Capnopen® and Triplepen with axial rotation were compared. The aerosol granulometry (MAD) was determined by laser diffraction spectrometry. The relative dye intensity and integrated density (RID) were analysed on a blotting paper with ImageJ® to assess the homogeneity of spatial distribution. Finally, we compared the tissue aerosol uptake in real-time and the tissue concentration of cisplatin and doxorubicin in the ex-vivo enhanced inverted bovine urinary bladder (eIBUB).
Results
To achieve the recommended upstream pressure >11bar, a flow of 3.4ml/s was needed for the Triplepen vs. 0.6ml/s for the Capnopen®, resulting in a shorter aerosolisation time (1.0 vs. 5.6min for 200ml). The aerosol droplet size (MAD) was smaller in the Capnopen® 35.6 (CI 34.5-36.6) vs. 43.2 (CI 28.0-58.4) (axial nozzle) and 42.3 (CI 39.3-45.3) and 45.5 (CI 37.6-53.5) µm (lateral nozzles) in the Triplepen. The spray pattern of the Triplepen had three spots but was inhomogenous (Fig. 1). Based on the RID, the staining was more homogeneous with Capnopen® (p≤0.001). Real-time tissue drug uptake did not differ significantly between Capnopen® vs. Triplepen (p=0.07). Cisplatin tissue concentration was 39% less after aerosolisation with the Triplepen vs. Capnopen® (14.4±6.3 vs. 23.4±9.2ng/ml, p<0.001). Similarly, Doxorubicin tissue concentration was lower in the Triplepen group (1.3±1.2 vs. 1.5±1.2ng/ml, p=0.47).
Conclusion
The Triplepen did not provide the expected results. Cisplatin (p<0.001) and Doxorubicin (ns) tissue concentrations were lower with the Triplepen vs. the Capnopen®. There was no clear advantage of the Triplepen concerning the homogeneity of blue ink staining and DOX tissue concentration ex-vivo. Technical and medical equivalence between the Triplepen and the CE-certified device (Capnopen®) could not be verified.