Intraoperative Systematic ICG Fluorescence Imaging in Reducing Anastomotic Leakage after Oesophagectomy with Gastric Tube Reconstruction – A Propensity-Score Matched Study
Authors
Fok, Chi Ying Jacquelyn1, Yip, Hon Chi2
Affiliations
- Department of Surgery, Prince of Wales Hospital, Hong Kong
- The Chinese University of Hong Kong, Hong Kong
Introduction
Anastomotic leakage is one of the major complications associated with esophagectomy. A major contributing factor is related to blood supply to the gastric tube. ICG (indocyanine green) fluorescence imaging aims to provide objective evaluation of gastric conduit perfusion before oesophagogastric anastomosis. This study aims to evaluate the benefit of intraoperative ICG perfusion assessment in reducing anastomotic leakage.
Methods
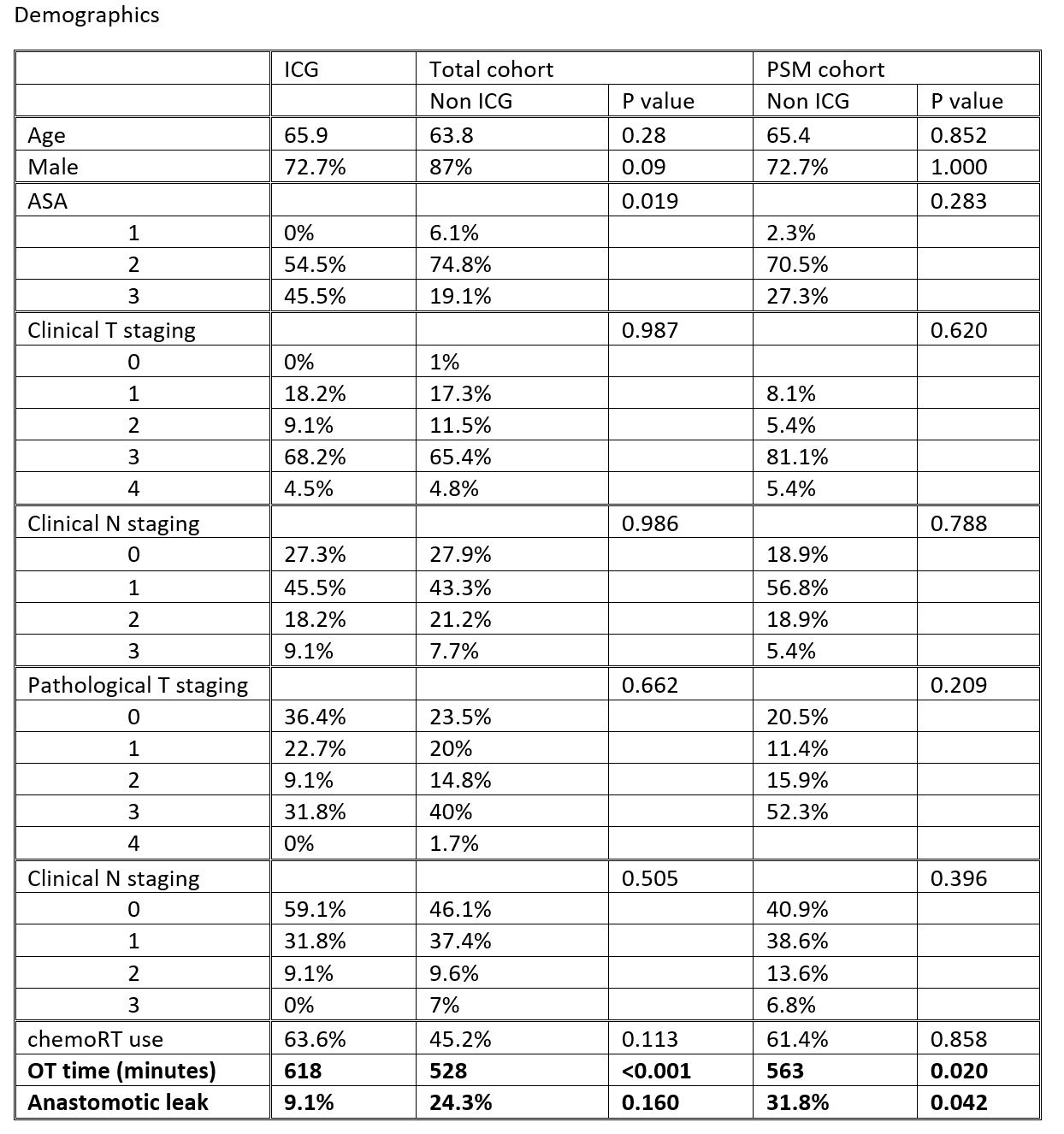
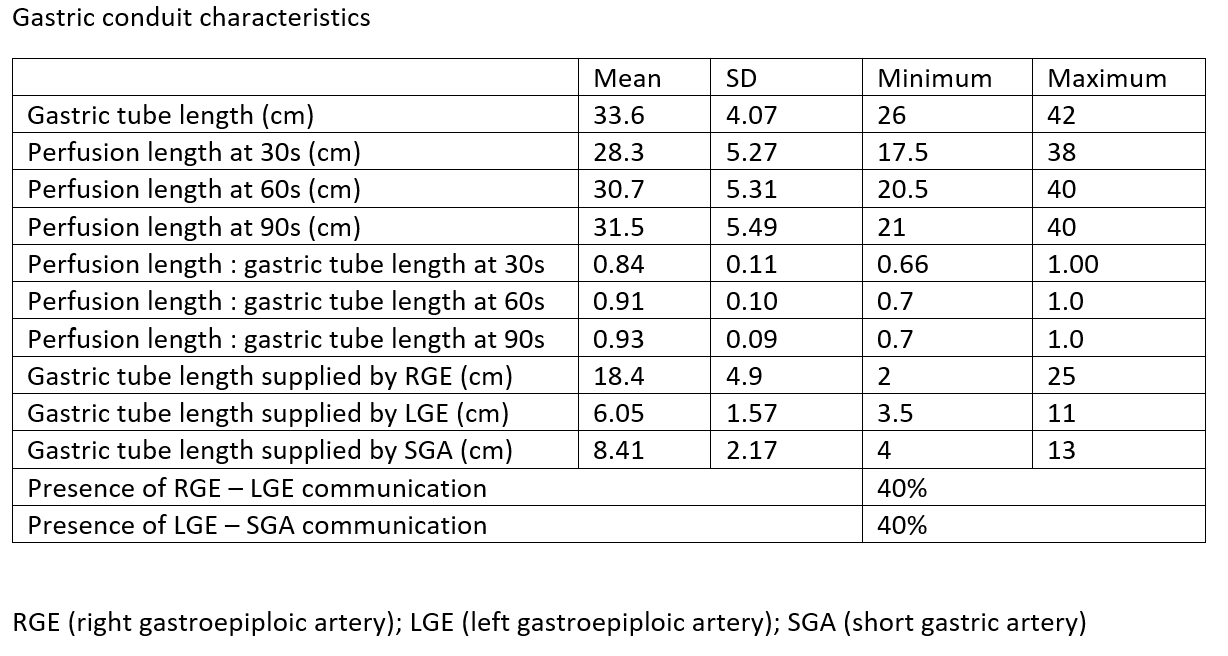
We prospectively evaluated 22 consecutive patients who underwent oesophagectomy with gastric conduit reconstruction with systematic intraoperative ICG fluorescence imaging evaluation. A 3cm gastric tube was fashioned. During the procedure, detailed evaluation of the gastric tube length as well as perfusion length at different time point was performed. The anastomosis was performed at preferably 30 second region, while gastric tube portion with >60 second perfusion time would be resected if suitable. This group was compared to a historical control of 115 patients before the introduction of standardized ICG use in our centre. Further analysis was done after 1:2 propensity score matching (PSM) of these two groups, which included 66 patients in total.
Results
The anastomotic leak rate was 9.1% in the ICG group vs 31.8% in the non-ICG group after PSM (p = 0.042). The operative time was significantly longer for the ICG group (618 vs 563 minutes, p=0.02). Within the ICG group, anastomosis at a site with ICG signal within 60 seconds of injection significantly reduces anastomotic leakage (p=0.001). Gastric tube length and perfusion length at different time points were not significant predictors of anastomotic leakage in this cohort.
Conclusion
Intraoperative systematic ICG fluorescence imaging improves perfusion assessment during oesophagectomy and reduces the risk of anastomotic leak in our cohort. Making an anastomosis at a site with ICG signal within 60 seconds of injection is preferrable. Further study with a larger sample size is recommended to prove these findings.