Evaluation and Comparison of Risk Stratification Systems for Gastrointestinal Stromal Tumor (GIST): A Multicenter Study
Authors
Miss Ruby Leung1, Mr. Steven Tsang1, Dr. Maximus Yeung2, Dr. Claudia Wong1, Dr. Desmond Chan1, Dr. Betty Law1, Dr. SY Chan1, Prof. Simon Law1, Dr. Ian Wong1
Affiliations
- Department of Surgery, School of Clinical Medicine, LKS Faculty of Medicine, The University of Hong Kong, Hong Kong SAR, China; rubylhc@connect.hku.hk (R.L), iyhwong@hku.hk (I.W.)
- Department of Pathology, School of Clinical Medicine, LKS Faculty of Medicine, The University of Hong Kong, Hong Kong SAR, China
Introduction
The Armed Forces Institute of Pathology (AFIP), the modified National Institutes of Health (NIH), and the American Joint Committee on Cancer (AJCC) TNM staging systems are widely used for prognostication in gastrointestinal stromal tumors (GIST). This study aimed to evaluate and compare the performance of these systems in risk stratification for GIST patients in Hong Kong.
Methods
Clinical data of patients with surgically resected GIST were collected and retrospectively analyzed from four hospital databases in Hong Kong between December 2013 and December 2021. Tumor size, mitotic count, primary tumor site, and tumor rupture incidence were evaluated. Risk stratification was performed using the AFIP, NIH, and AJCC systems. Overall survival (OS) and recurrence-free survival (RFS) were analyzed using Kaplan-Meier curves, compared by Log-rank test. Logistic regression was used to determine factors affecting recurrence.
Results
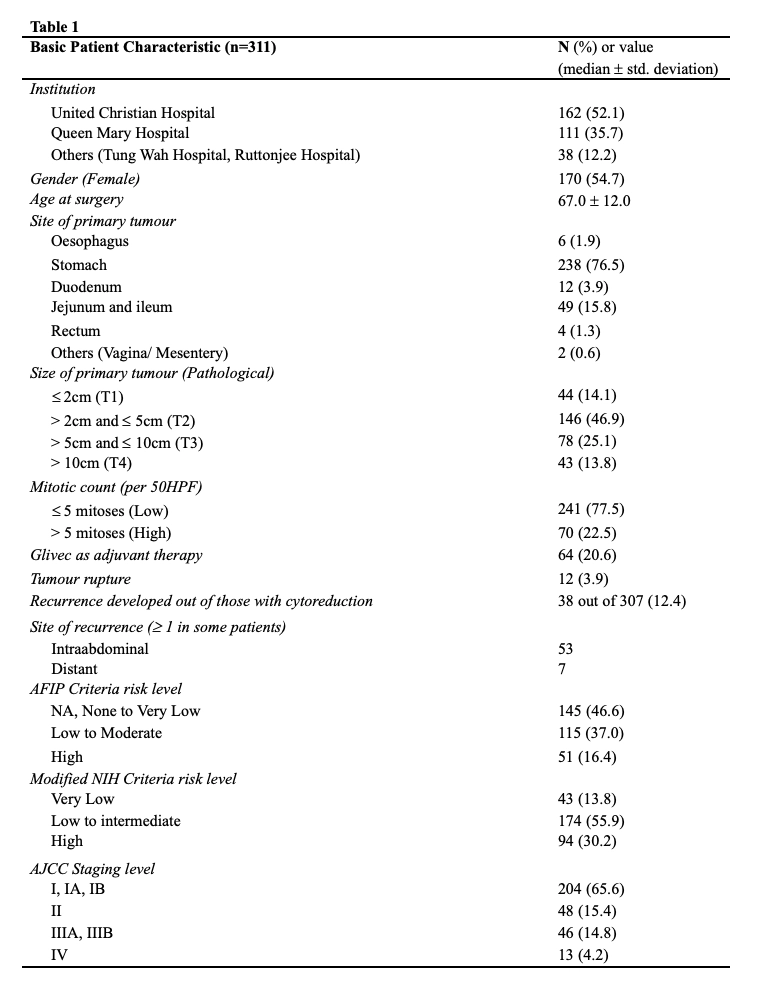
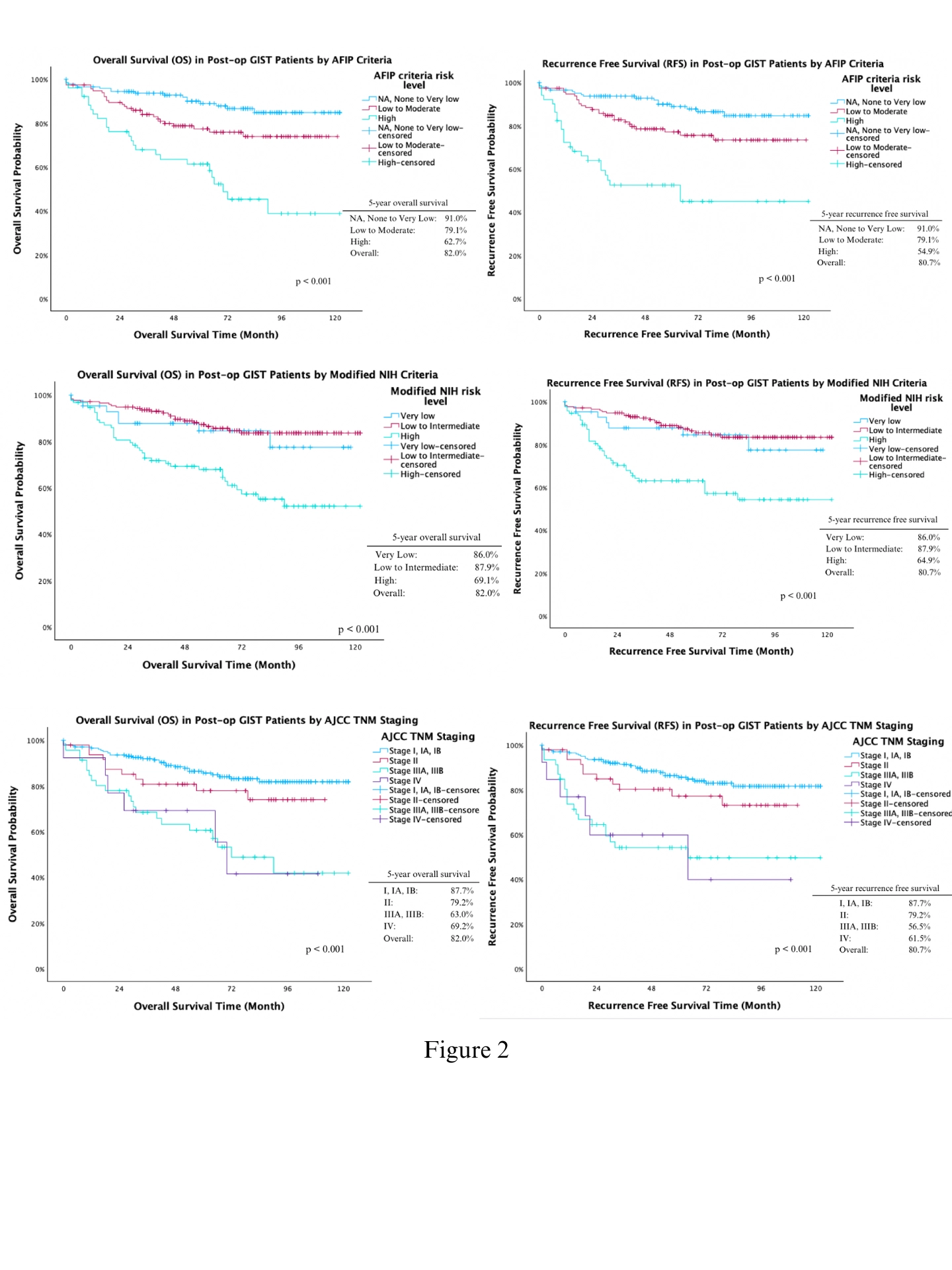
A total of 311 GIST patients were identified over the past 8 years. (Figure 1) The AFIP criteria accurately predicted decreasing OS and RFS with increasing risk category (OS/RFS: 110/110, 97.8/97.2, 72.0/66.5 months; P<0.001). The remaining two systems generally stratified patients into two groups. For modified NIH criteria, very-low and low-to-intermediate risk groups showed similar OS and RFS (OS/RFS: 101/101, 108/108, 81.6/77.9 months; P<0.001). AJCC staging mostly followed the expected trend, with higher stages associated with worse outcomes, while stage III and IV showed similar OS and RFS (OS/RFS: 107/107, 91.1/90.5, 73.6/70.0, 68.8/60.4 for stages I, II, III, IV; P<0.001). (Figure 2) Those without tumor rupture had longer survival than those with tumor rupture (OS: 101 vs 61.7 months, P<0.001). Among highrisk patients, the use adjuvant Imatinib significantly improved survival compared to non-use (OS: 86.7 vs 49.5 months, p=0.014). Male had a 2.12 times higher recurrence risk than female (p=0.032).
Conclusion
The AFIP criteria performed the best in stratifying risk for GIST patients in Hong Kong.